Maxillary expansion or bicuspid extraction: A case study in orthodontics
By
To pull or not to pull? . . . the decision to extract permanent teeth in an adult patient is not always an easy one. When an adult patient presents with severe crowding and a posterior crossbite, will dental and skeletal expansion create sufficient space to resolve the crowding, or will teeth need to be extracted as well? This question can be answered by predicting the amount of space that can be gained with dental and skeletal expansion, keeping in mind the desired esthetic outcome and overall oral health of the patient. A study performed by Adkins et al., found that the amount of arch length created by first premolar expansion can be calculated by multiplying the amount of expansion to be preformed by a factor of 0.7. (1) How do we determine how much expansion is appropriate so that we can calculate the amount of space to be gained?

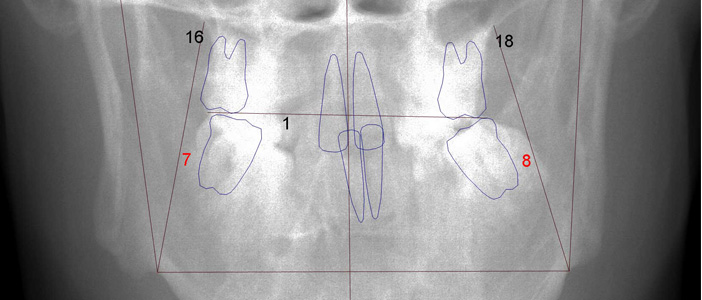
By using a frontal cephalogram (figure 1), we can determine the amount of skeletal expansion that is required for the maxillary arch to achieve the proper width to match the mandibular arch. To calculate the increase in space, however, we need to calculate the removal of any dental tipping in addition to the skeletal expansion. There are two processes that often occur simultaneously when correcting a posterior crossbite. One process is to remove all dental tipping so that each tooth is centered over the supporting bone. The other process is to correct any transverse maxillary skeletal deficiency. Haas noted that expansion of the maxilla can result in making upright, lingually tipped, lower-arch teeth without lower fixed appliances. (2) It is important to note that it is easy to misdiagnose a skeletal posterior crossbite when the maxillary posterior teeth are tipped facially and the mandibular posterior teeth are tipped lingually—when evaluating a crossbite by dental relationships only. Once the posterior teeth are upright, the maxillary transverse skeletal deficiency can be visualized and match the diagnosis provided by a frontal cephalogram. Let us explore the process of evaluating a patient for dental extractions, using a case study that demonstrates severe crowding and transverse skeletal discrepancy.
A 28-year-old male presented with a chief complaint that he avoided smiling due to his canines that “stick out” (figure 2).

Rickett’s Analysis showed a mesio-facial face type and skeletal Class I relationship. His interincisal angle was 132 degrees, which is ideal. His mandibular arch demonstrated a severe curve of Wilson, while the maxillary arch demonstrated a left side posterior crossbite. The left side occlusion was full Class II at the molars and Class I on the right side. Total maxillary crowding was calculated at 12 mm and mandibular at 7 mm. No missing teeth were observed. Mandibular arch width from first molar central groove to central groove was 39 mm. From lingual cusp to lingual cusp of the maxillary first molars, the arch width was 32 mm. Due to the crowding and narrow maxillary arch, the smile arc was uneven (figures 3 and 4).


Using the patient’s lower-arch model, it was determined that the true lower arch width at the first molars was 46 mm by visualizing the lower posterior teeth fully centered over the alveolus. Using Rickett’s Analysis on the patient’s frontal cephalogram, the lower molars were tipped too lingually by three standard deviations. The mandibular width according to Rickett’s measurements, was initially 84.5 mm and ideally would be 91.6 mm. Both manners of measuring the lower arch width showed the need to expand the lower posterior teeth by 7 mm. Thus, it was determined that the lower molars needed to be expanded from a width of 39 mm to 46 mm, and the maxillary arch needed to be expanded dentally and then skeletally from 32 mm to 46 mm. The lower arch acted as the template to which the maxillary arch should be expanded to match (figures 5 and 6).

As noted above, using the factor determined by Adkins et al., 0.7 times 14 mm of maxillary dental and skeletal expansion provides approximately 10 mm of space to aid with resolving the 12 mm of maxillary arch length deficiency. Distalizing the left side maxillary posterior teeth to correct the occlusion provided an additional 4 mm of space. Considering the space gain from expansion and distalizing the upper left quadrant to correct the occlusion, it becomes clear that extractions are not mandatory to resolve this patient’s crowding, and a nonextraction treatment option is available.

Even though the calculations determine sufficient space can be created to resolve this patient’s crowding with expansion of the posterior teeth, the question remains: Is nonextraction treatment the ideal treatment for this patient? Without removing teeth, it could be argued that there is an increased risk that the patient may require gingival grafting, which ended up being a reality in this case. Also, to achieve this level of expansion, the patient must go through a surgical procedure to attain the desired amount of expansion. The final decision should then be brought back to the patient. When the option of teeth extraction versus expansion were provided, discussing the advantages and disadvantages of both options, the patient preferred to go through the surgical procedure rather than have teeth extracted. The benefit of this course of treatment is a fuller smile that fits the patient’s true lower arch width.

Surgically assisted rapid maxillary expansion (SARPE) is a procedure whereby an oral surgeon performs a maxillary Le-Fort I osteotomy minus the down fracture of the maxilla. This frees the two segments of the maxilla for minimally restricted expansion. Suri and Taneja report that for cases with maxillary transverse deficiency (MTD), “the incidence of MTD in the adult population or in skeletally mature people could not be elucidated from the literature.” (3) The authors do provide guidance that in a skeletally mature patient, “when the MTD is greater than 5 mm, surgical assistance is essential.” (3) In this case the MTD was 9 mm, indicating the need for SARPE. Rapid maxillary expansion, surgically assisted or not, is notoriously unstable—making retention of the expansion movements essential. In a study by Petrick et al., patients who underwent SARPE treatment did not have sufficient bone density of the midpalatal suture up to seven months postsurgical procedure to maintain the surgical expansion. (4) Applying this information in this case, a transpalatal arch was used throughout treatment to assure maintenance of the achieved transverse expansion. When transitioning from the expander to the transpalatal arch, the expander was left in place on the maxillary first molars, while the TPA was fabricated for the maxillary second molars. Thus, arch width retention was present during active treatment with fixed appliances until finishing mechanics were applied (figure 7).

Extracting teeth in this patient would have collapsed the dental arches to a significant degree and simply compensated for the true skeletal discrepancy. It is reasonable to assess that crossbite correction may not have been achievable with extraction treatment alone, even with dental tipping. Additionally, there is a growing awareness of the effects of orthodontic treatment on a patient’s risk for sleep apnea. Wertz reported finding an increase in the nasal airway when a patient’s maxillary arch was expanded. (5) When the opportunity to increase a patient’s airway presents, it should be considered carefully. Moreover, extracting teeth can reduce the space for a patient’s tongue. This can affect the stability of the orthodontic result as well as encourage a more posterior tongue placement encroaching on the airway. Measuring dental and skeletal archwidth is necessary for proper diagnosis and may avoid unnecessary need of dental extractions. Even in cases demonstrating less dental crowding and mildly narrow maxillary arches, expansion allows for ideal vertical contact of posterior teeth without any lingual or buccal tipping of the posterior teeth as compensation (figure 8).
 Tyler Pritchard, DDS, earned his DDS degree from Loma Linda University in 2006. After graduating from dental school, he attended a general practice residency at the Loma Linda Veterans Hospital for one year. He completed his orthodontic residency in September 2009, earning a master’s degree from Loma Linda University. Dr. Pritchard is a second-generation orthodontist and a third-generation dentist. He practices orthodontics in Battle Ground, Washington.
Tyler Pritchard, DDS, earned his DDS degree from Loma Linda University in 2006. After graduating from dental school, he attended a general practice residency at the Loma Linda Veterans Hospital for one year. He completed his orthodontic residency in September 2009, earning a master’s degree from Loma Linda University. Dr. Pritchard is a second-generation orthodontist and a third-generation dentist. He practices orthodontics in Battle Ground, Washington.
References
1. Adkins MD, Nanda RS, Currier GF. Arch perimeter changes on rapid palatal expansion. Am J Orthod Dentofacial Orthop. 1990;97:194–199.
2. Haas AJ. Long-term post-treatment evaluation of rapid palatal expansion. Angle Orthod. 1980;50:189–217.
3. Suri L, Taneja P. Surgically assisted rapid palatal expansion: A literature review. Am J Orthod Dentofacial Orthop.2008;133:290–302.
4. Petrick S, et al. Bone density of the midpalatal suture 7 months after surgically assisted rapid palatal expansion in adults. Am J Orthod Dentofacial Orthop. 2011;139:S109–116.
5. Wertz RA. Skeletal and dental changes accompanying rapid midpalatal suture opening. Am J Orthod. 1970;58:41–66.
Looking for an orthodontist in Beaverton, Oregon? Biermann Orthodontics is a cutting-edge orthodontic practice that serves Beaverton and Molalla, OR, and focuses on providing world-class customer service and efficient treatment. We strive to create stunning smiles in the shortest amount of time without ever sacrificing quality.
Visit our Locations page to find a clinic near you, or schedule an initial consultation.
Biermann Orthodontics
503-690-0722
17885 NW Evergreen Parkway, Suite 200
Beaverton, OR 97006